
One of the largest opportunities to reduce waste in Medicare isn't hidden in a complex payment model; it's sitting in plain sight.
Every year, hundreds of thousands of Medicare beneficiaries receive injections to treat age-related macular degeneration and diabetic eye disease. The most commonly used branded drugs cost between $1,250 and $2,500 per dose. Yet a clinically comparable alternative, bevacizumab (Avastin), costs roughly $70 per dose. Multiple landmark studies have shown similar visual outcomes for many patients.
The Economics of Waste
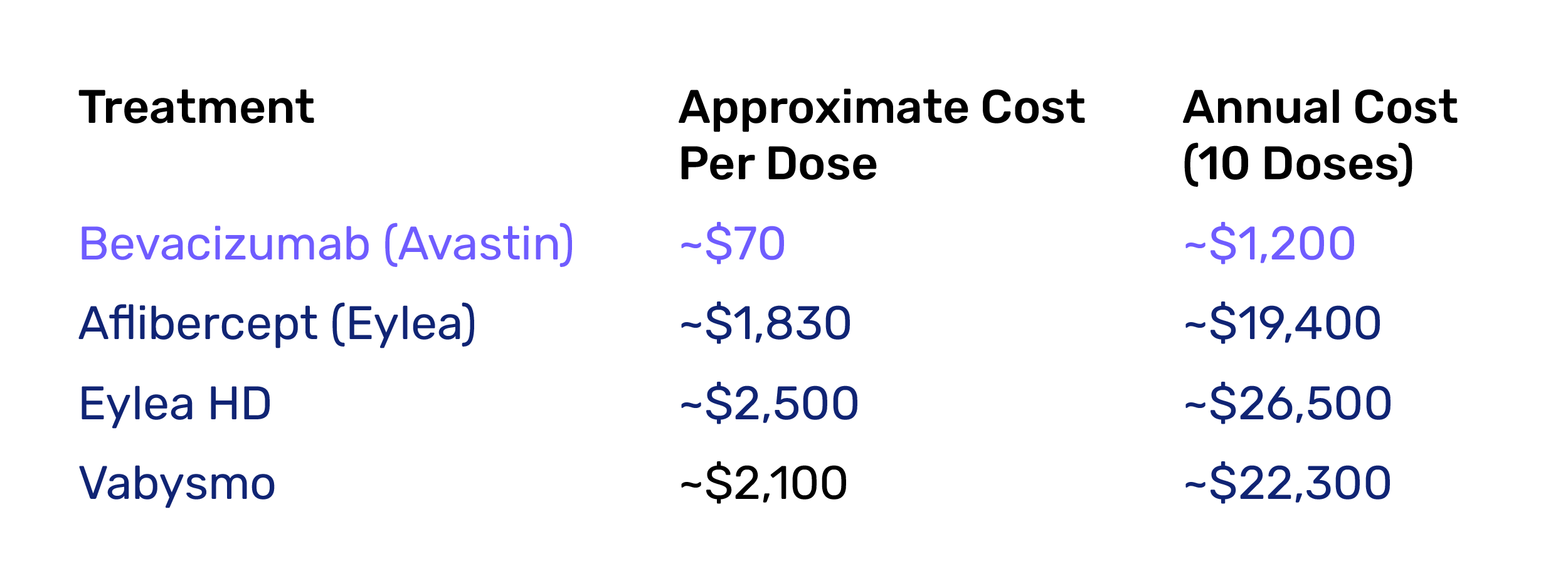
For a typical patient who could get similar benefits from the generic as from the branded drug, Medicare can spend $18,000–$25,000 more per year than necessary. This could result in as much as $3-$5B of waste per year.
The reason isn't necessarily clinical; it is confounded by economic incentives. Under Medicare's buy-and-bill system, specialists earn substantially more revenue from higher-cost drugs (e.g., ~6% on drugs they administer), creating incentives that favor expensive therapies even when lower-cost alternatives are appropriate, purely as a mathematical artifact of multiplying the percentage against a larger number.
The solution isn't simply restricting choice. It is aligning incentives. By sharing savings with specialists who deliver equivalent outcomes at lower cost, value-based care models can preserve physician economics, protect patient vision, and return thousands of dollars per patient back to Medicare.
This is exactly the type of waste America can no longer afford. The goal isn't cheaper care. The goal is better care at a rational price.
- Chakravarthy U, Harding SP, Rogers CA, et al; IVAN Study Investigators. Alternative treatments to inhibit VEGF in age-related choroidal neovascularisation: 2-year findings of the IVAN randomised controlled trial. Lancet. 2013;382(9900):1258-1267.
- Jhaveri CD, Glassman AR, Ferris FL III, et al; DRCR Retina Network. Aflibercept monotherapy or bevacizumab first for diabetic macular edema. N Engl J Med. 2022;387(8):692-703.
- Maguire MG, Martin DF, Ying GS, et al; Comparison of Age-Related Macular Degeneration Treatments Trials (CATT) Research Group. Five-year outcomes with anti-vascular endothelial growth factor treatment of neovascular age-related macular degeneration: the Comparison of Age-Related Macular Degeneration Treatments Trials. Ophthalmology. 2016;123(8):1751-1761.
- Martin DF, Maguire MG, Ying GS, Grunwald JE, Fine SL, Jaffe GJ; Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N Engl J Med. 2011;364(20):1897-1908.
- Martin DF, Maguire MG, Fine SL, et al; Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology. 2012;119(7):1388-1398.
- Wells JA, Glassman AR, Ayala AR, et al; Diabetic Retinopathy Clinical Research Network. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med. 2015;372(13):1193-1203.
- Wells JA, Glassman AR, Ayala AR, et al; Diabetic Retinopathy Clinical Research Network. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema: two-year results from a comparative effectiveness randomized clinical trial. Ophthalmology. 2016;123(6):1351-1359.
Pearl Health is powering the future of healthcare
We’re a team of physicians, technologists, and risk-bearing experts with a passion for enabling our partners to deliver better care and reduce health system costs. Want to learn more?

