
The Long-term Enhanced ACO Design (LEAD) Model represents CMMI’s most ambitious step in value-based care: a 10-year framework designed to enable sustained investment in care coordination, especially for high-needs, homebound, and dually-eligible populations.
We applaud CMMI for incorporating ACOs’ feedback and including many new innovative changes, but LEAD risks carrying forward a critical flaw from the REACH model - prohibiting Durable Medical Equipment (DME) providers’ ability to participate as Preferred Providers.
Why This Matters
LEAD’s core mechanism is simple: align financial incentives with outcomes. Preferred Providers can participate in risk-sharing arrangements like the Advanced Payment Option (APO) and Non-Primary Care Capitation (NPCC), driving coordination, accountability, and proactive care.
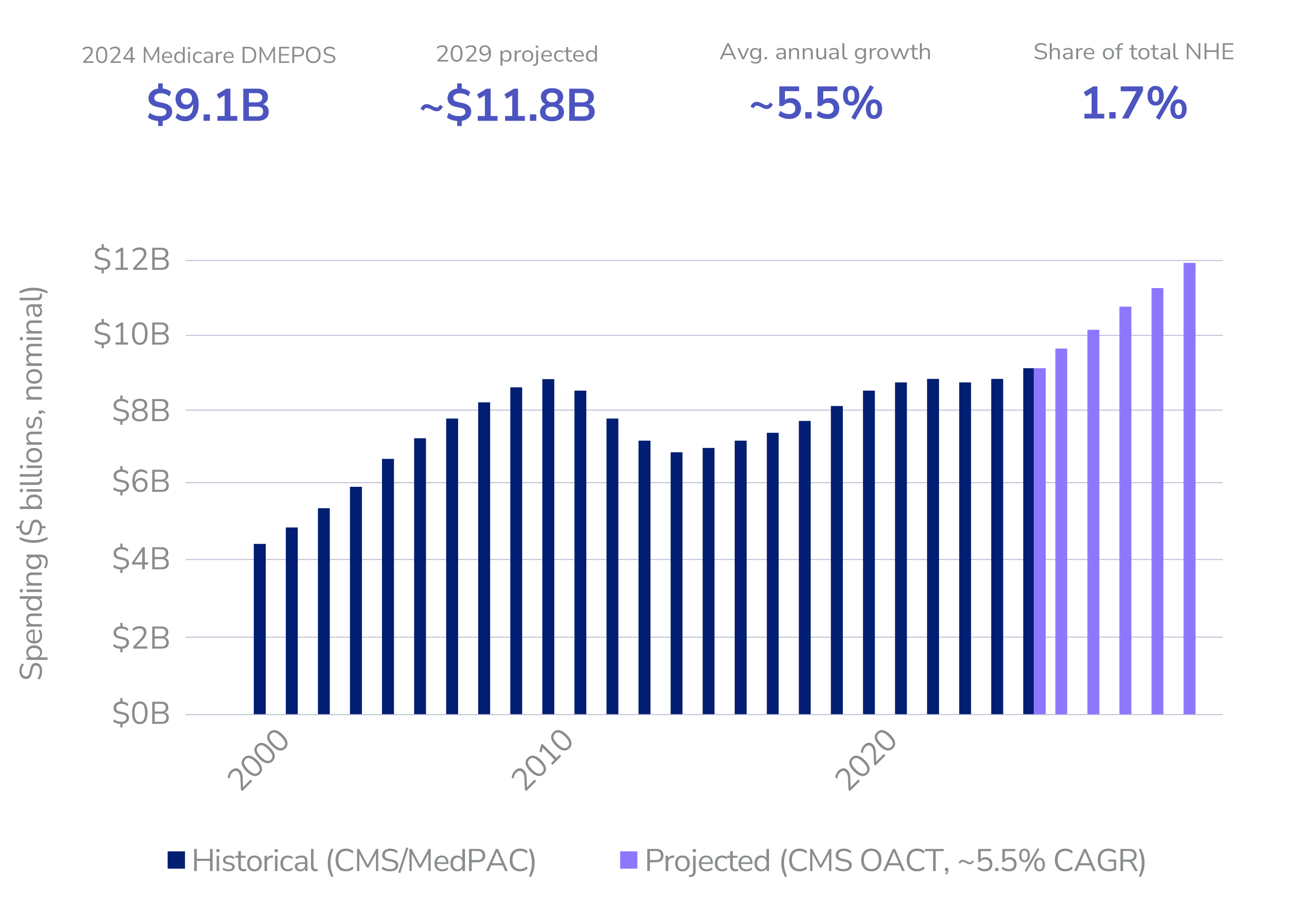
DME providers sit entirely outside this risk structure today: paid fee-for-service with no accountability for outcomes and no formal integration with ACO care teams. Durable Medical Equipment (DME) represents approximately 1.5% to 1.7% of total Medicare spending. As of recent 2024 projections, this expenditure equals roughly $9.1 billion, with spending projected to exceed $12 billion by 2030.
DME Is Central to LEAD’s Target Population
LEAD prioritizes patients with complex, chronic conditions, and those most dependent on home-based care. For these patients, DME is not ancillary; it’s foundational.
Oxygen therapy, CPAP, wound care devices, mobility support, and diabetic supplies directly determine whether patients remain stable at home or return to the hospital. Delays, mismanagement, or poor coordination in DME are well-documented drivers of readmissions and avoidable utilization.
If LEAD is serious about reducing hospitalizations and improving “days at home,” DME cannot remain outside the accountability framework.
What Changes If DME Is Included
1. Incentives Drive Behavior
Allowing DME providers to participate in APO or other risk arrangements aligns them with ACO and CMMI goals. Instead of being paid for volume, they become accountable for outcomes, motivating investment in timely delivery, patient education, adherence monitoring, and real-time coordination.
2. Care Coordination Becomes Structural, Not Optional
Today, DME relationships are transactional. Inclusion in LEAD would enable formal workflows, shared data, and accountability across providers: bringing DME into the care team rather than leaving it as a disconnected vendor.
3. Readmissions Can Be Directly Reduced
DME failures are a known driver of readmissions in CHF, COPD, and post-acute populations. Aligning DME providers financially with ACO performance creates a powerful lever to close this gap.
Addressing the Real Concern: Fraud
As most know, DME has been a significant source of Medicare fraud, waste, and abuse. That concern is valid and it is the primary reason for exclusion.
But exclusion is a blunt instrument that sacrifices clinical and economic value and blocks one of the best fraud detectors in Medicare: ACOs.
A better approach is controlled inclusion:
- Restrict participation to accredited, high-performing suppliers
- Apply rigorous vetting and monitoring (as done with all other providers)
- Use data-sharing and claims analytics to detect anomalies in real time
- Enable ACOs to flag participating and non-participating DME vendors for potential fraud cases.
Importantly, bringing DME inside ACO financial models turns ACOs into active fraud detectors. When ACOs are at risk for total cost of care, they have strong incentives to identify inappropriate utilization, billing irregularities, and low-value suppliers. They contract with higher quality partners and leave fraudulent ones out.
In other words: APO + accountability does not increase fraud risk; it creates aligned entities with the incentive and data to reduce it.
The Time Is Now - Not Ten Years From Now
LEAD’s 10-year horizon changes the investment equation. It enables ACOs and DME providers to build durable infrastructure: shared data systems, protocols, and accountability mechanisms that shorter models could not support.
CMMI is already advancing structured risk relationships through a broader swath of the healthcare provider landscape via CMS-Administered Risk Arrangements (CARAs) in LEAD. Extending that logic to DME is consistent, not radical.
Critically, CMMI seems to agree, as the recently released LEAD RFA hints at future innovations between ACOs and DME suppliers, via a potential benefit enhancement:
“Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) Flexibility: DMEPOS are essential tools that enable beneficiaries to manage chronic conditions, recover from acute episodes, and maintain independence in their daily activities. However, administrative requirements currently create delays that can impede timely access to medically necessary equipment. High Needs beneficiaries, who use DMEPOS more than the general Medicare population, are particularly impacted by these requirements. CMS is exploring options to support improved access to DMEPOS in the model” - LEAD RFA. Section VII.E.4. Benefit Enhancements and Beneficiary Engagement Incentives Under Consideration
What CMMI Should Do: A New Type of RACI
Nevertheless, the details of this potential flexibility remain unclear. We would suggest CMMI examine program features that empower ACOs and Medicare beneficiaries:
- Ramp: Consider a phased or piloted approach with defined evaluation metrics
- Accountability: Allow participation in APO and other risk-based arrangements
- Compliance: Establish clear standards for data sharing, care coordination, and compliance
- Inclusion: Reclassify qualified DME providers as eligible ACO Preferred Providers
Bottom Line
LEAD is designed to bend the cost curve through innovative, coordinated, accountable care. That goal is harder to achieve if one of the most clinically impactful provider categories remains outside the model.
DME providers should not be excluded. They should be carefully integrated.
With the right guardrails, inclusion doesn’t just improve care, it strengthens program integrity by aligning incentives and enabling ACOs to actively detect and reduce fraud.
Pearl Health is powering the future of healthcare
We’re a team of physicians, technologists, and risk-bearing experts with a passion for enabling our partners to deliver better care and reduce health system costs. Want to learn more?

